

How Accurate Are Covid Numbers?
How Accurate Are Covid Numbers?
Were we truly in a pandemic? Has Covid been one giant IQ test?

If you have not read The Truth About Covid: Parts 1-4 of this series, I highly suggest doing so.
If you want to know what’s coming to the U.S. in the coming weeks and months, I highly suggest reading my article: Freedom vs. Dystopian Hell
The great enemy of truth is very often not the lie--deliberate, contrived and dishonest--but the myth--persistent, persuasive and unrealistic. Too often we hold fast to the cliches of our forebears. We subject all facts to a prefabricated set of interpretations. We enjoy the comfort of opinion without the discomfort of thought. - JFK
There is nothing more permanent than a temporary government program. - Ronald Reagan
Introduction:
During the duration of the Covid pandemic, one variable has remained constant: the persistent portrayal and discussion of the numbers associated with Covid, from case numbers, to hospitalization numbers, death numbers and more recently vaccine numbers. For the last 18 months, the numbers associated with Covid have been placed front and center on every news outlet. The public has been conditioned into a state of fear due to the constant sight and discussion of Covid numbers. This reiteration and emphasis of numbers have psychologically conditioned individuals to fear life itself. In this article I will provide insight into the unprecedented changes made by the CDC, to the guidelines for reporting deaths exclusively for Covid. I will also highlight the ICD-10 hospital coding system and discrepancies that surround death certificates attributed to Covid. The premise behind this article is to provide justification behind the possibility of inflated Covid numbers that have driven the narrative of the pandemic. Information I provide will show that there is reason to believe that the numbers are inaccurate and have been heavily inflated. I’ll leave you with this question: Were we ever truly in a pandemic?
How Are The Numbers Reported?
A study published in The Institute for Pure and Applied Knowledge highlighted major discrepancies in regards to Covid related case and death numbers reported. These discrepancies arose as a result from changes the CDC made to the reporting guidelines, exclusively for Covid. The study included various federal laws that were broken by the CDC from the implementation of said changes. I included this article in part 3 of my Truth About Covid mini-series but the information provided is relevant to understanding the premise of this article. Let’s take a look at the changes made to reporting guidelines and the effects said changes have had on the numbers presented to the public.
COVID-19 Data Collection, Comorbidity & Federal Law: A Historical Retrospective

In 2003, the CDC published the CDC’s Medical Examiners’ & Coroners’ Handbook on Death Registration and Fetal Death Reporting and the CDC’s Physicians’ Handbook on Medical Certification of Deaths. These guidelines had been place for 17 years and been proven to be effective without flaw. Both of these handbooks became the nationwide standard regarding the methods of how cause of death is recorded for cases involving comorbidity on death certificates. Interestingly, these handbooks remain to be the method of recording for all causes of death except in cases where Covid-19 is suspected or confirmed.

On March 24th, 2020: The National Vital Statistics System (NVSS) was advised by the CDC to issue “COVID-19 Alert No. 2” to all physicians, medical examiners and coroners. These guidelines led to the alteration of how cause of death are reported on death certificates, exclusively for Covid-19. These changes significantly altered how deaths were to be reported. It is extremely important to understand the significance of this change because the numbers reported in the last 18 months are under a set of guidelines that have never been used before.
NVSS COVID-19 Alert No. 2 Guidelines vs. 2003 Guidelines:
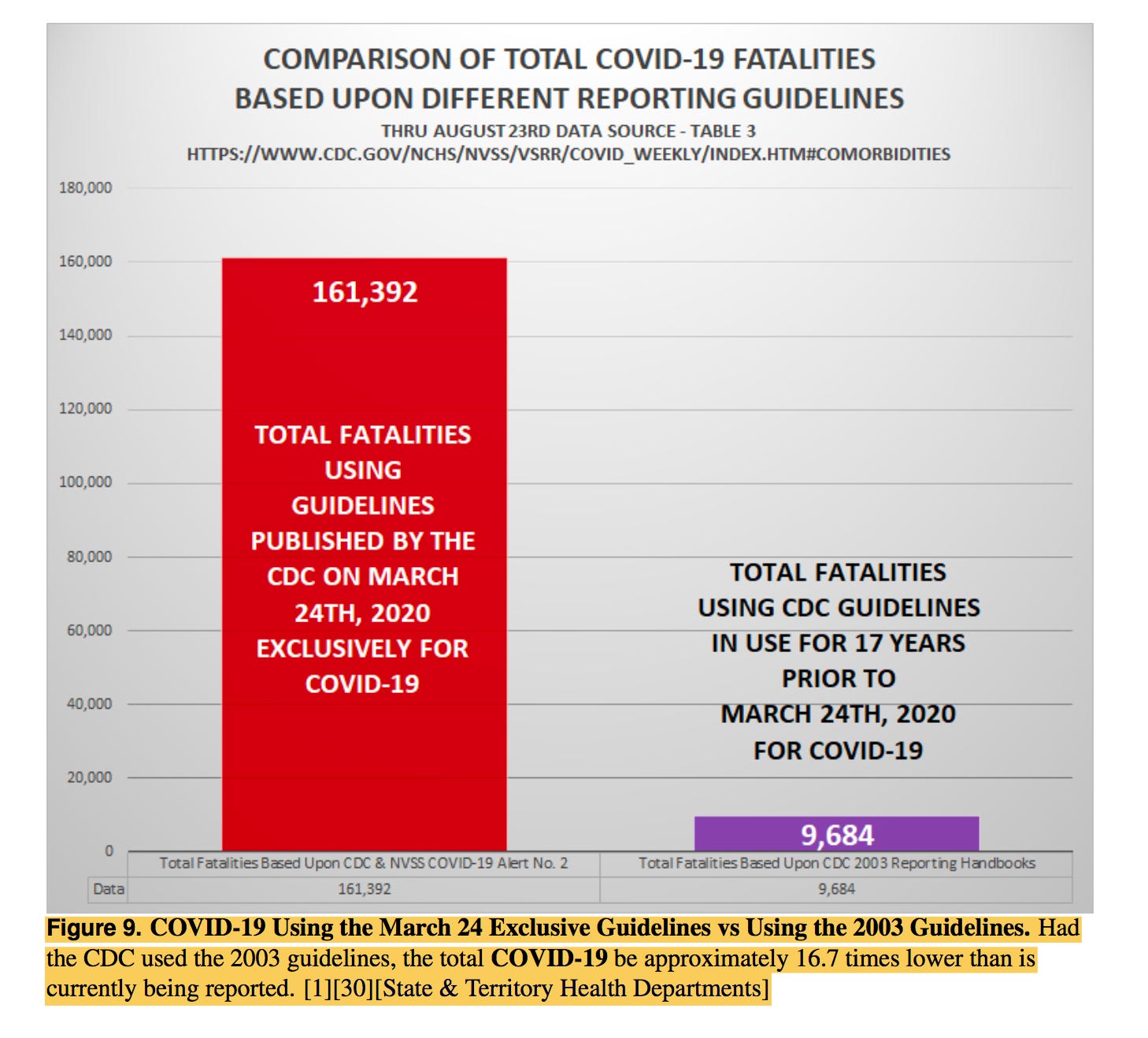
The effect on the number of deaths attributed to Covid as a result from these changes is rather significant. This bar chart shows the massive inflation of Covid related deaths that have resulted from the changes that were made to the guidelines. The total difference between the March 24th changes and the 2003 guidelines is 151,708 listed fatalities. This number is astronomical given the alleged accuracy of the numbers reported during the timeframe presented in this study.
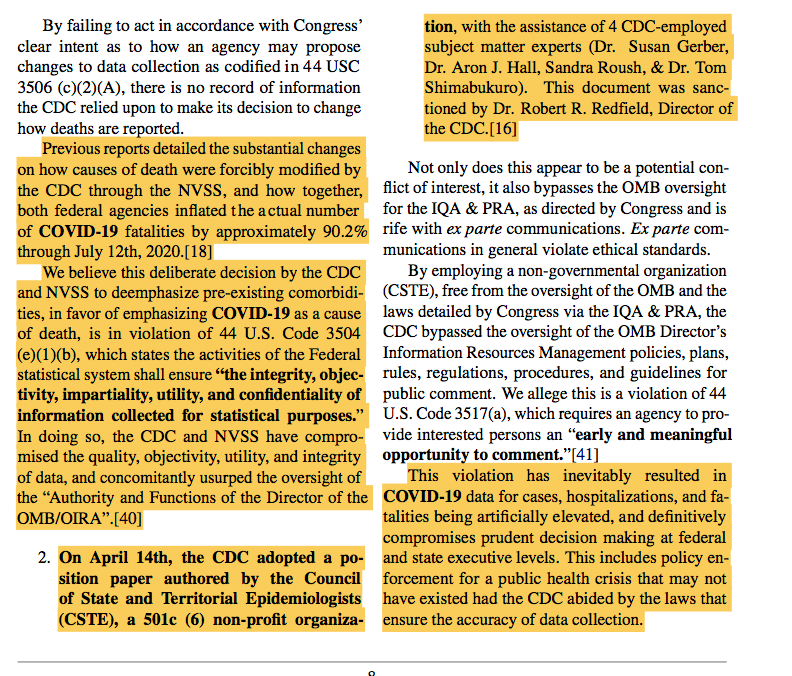
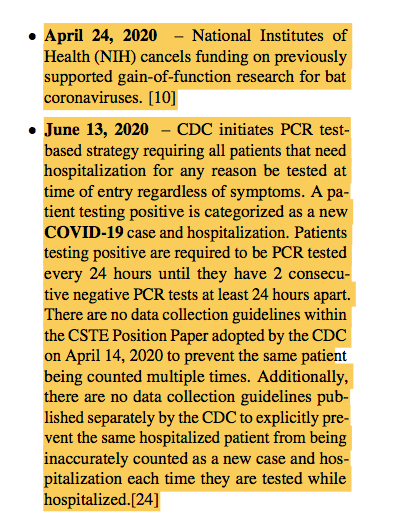
On April 14th, 2020: The CDC changed the medical criteria for diagnosis solely for Covid-19 based on the CSTE Covid-19 position paper. The adoption of this paper altered the standard of established medical criteria used for diagnosis and bypassed federal oversight. The position paper was written by the Council of State and Territorial Epidemiologist (CSTE) which is a 501c non-profit organization. Four CDC-employed subject matter experts aided in the adoption of this paper which was sanctioned by the CDC director at the time, Dr. Robert Redfield. Keep in mind, former CDC Director Redfield continues to support the Wuhan lab leak theory. Voldemort Fauci and the NIH funded the gain of function research in Wuhan with taxpayer money, which has conclusively been proven. Those who continue to believe the wet market bat story have the intellectual capacity of a goldfish. Just wait until the masses realize that Covid was in the country as early as late October/early November of 2019 due to the World Military Games.
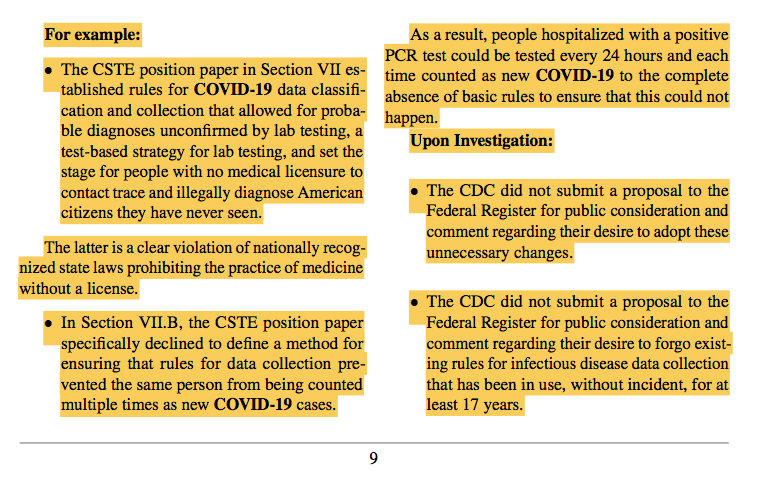
On June 13th, 2020: The CDC began the PCR test-based strategy which required all patients in need of hospitalization, to undergo a PCR test prior to admission, even if symptoms were not present. This means that EVERY patient admitted to the hospital regardless of reason, was forced to take a PCR test before admission to the hospital. An individual could have a heart attack or been in a wreck and prior to receiving hospitalized treatment, are forced to take a PCR test. If a patient tested positive, they were required to be tested every 24 hours until they produced two consecutive negative tests at least 24 hours apart. The CSTE paper adopted on April 14th included no data collection guidelines in regards to the classification of a positive case, which means nothing would keep an individual from being counted as a positive test more than once. The CDC also failed to publish additional guidelines that would prevent hospitals from recording the same patient as a new case and hospitalization following each test conducted. Hypothetically speaking, if an individual produced five consecutive positive tests prior to the required two consecutive negative tests, five new positive cases would have been recorded. As one can see, this is a very accurate method of recording. Keep in mind, the faulty PCR tests have been proven to be unreliable and have a 97% false positive rate when the cycle threshold is above 35 cycles which is lower than the FDA suggested “positive specimen” threshold. According the the FDA: “A specimen is considered positive for 2019-nCoV [virus] if all 2019-nCoV marker (N1, N2) cycle threshold growth curves cross the threshold line within 40.00 cycles ([less than] 40.00 Ct).” Part 4 of my series highlights the unreliability of the PCR tests.
As one can see, the changes made by the CDC without federal oversight suggest major issues in regards to the methods in which cases and deaths are to be reported. These changes alone have had a major contribution to the pandemic narrative and suggest that the numbers provided by officials are highly inflated. Knowing this information implies we do not know what the true number of cases and deaths FROM and involving Covid truly are. The discrepancies in the method of recording deaths, bring rise to the question: Were we ever truly in a pandemic?
ICD-10 Coding for Hospitals:
This section will help wrap everything in the previous section together and provide clarity behind the inflated death totals associated with Covid. Death Certificates at hospitals are assigned ICD-10 codes for diagnosis and the ICD-10 code for Covid is U07.1. Keep in mind, the CDC changed reporting guidelines exclusively for COVID-19. During the year 2020, approximately 375,000 U.S. deaths were attributed to COVID-19 or at least included the code U07.1 on the death certificate. The CDC had an interesting report posted online on March 31st, 2021 which summarized death certificates and the ICD-10 codes for diagnosis for Covid mortality. Findings from the report suggest that the COVID-19 mortality surveillance used on official death certificates present the possibility of heavily inflated death totals. Oddly enough, the report was published to “justify the accuracy ” of the mortality surveillance but in turn, did quite the opposite. To understand this section, one must understand the definitions of the words ‘from’ and ‘with.’
Among 378,048 death certificates from 2020 listing COVID-19, 5.5% list COVID-19 WITHOUT codes for any other conditions. Among 357,133 death certificates had at least ONE other condition, 97% had a co-occurring diagnosis of a plausible chain-of-event condition (e.g., pneumonia or respiratory failure), or a significant contributing condition(e.g., hypertension or diabetes), or both.
Make note of the important aspects in this excerpt from the report, 5.5% of the deaths listed Covid (U07.1) as the sole cause of death with no other conditions. Meaning that 5.5% (20,915) of the listed deaths were solely attributable to Covid, thus dying FROM Covid. In turn, 94.5% (357,133) of the death certificates that included the U07.1 code, also included another ICD-10 code meaning another contributing cause of death played a factor thus dying WITH Covid (allegedly, those PCR tests…).
Overall, 97.3% of 357,133 death certificates with at least one other diagnosis (91.9% of all 378,048 death certificates) were noted to have a co-occurring diagnosis that was a plausible chain-of-event conditions (e.g., pneumonia or respiratory failure), a significant contributing condition (e.g., hypertension or diabetes), or both. Overall, 70-80% of death certificates had both a chain-of-event condition and a significant contributing condition or a chain-of-event condition only; this was noted for adults aged 18-84 years, both males and females, persons of all races and ethnicities, those who died inpatient and outpatient or emergency department settings, and those whose manner of death was listed as natural.
As this excerpt reiterates, a significant majority of death certificates included a significant contributing condition and or a plausible chain-of-event condition. Just because U07.1 was included on the death certificate, does not mean we can conclude Covid was the actual cause of death. Like I previously mentioned, there is a definitive difference between dying FROM Covid and dying WITH Covid.
Death certificates were processed using standard CDC protocols to convert all written text and diagnoses to ICD-10 codes (4). Individual data elements were extracted for analysis from death certificates that had the ICD-10 code for COVID-19 (U07.1) listed in Part I (the section for reporting chain of events leading directly to death, the immediate cause of death, and the underlying cause of death) or Part II (the section for reporting all other significant conditions that contributed to death) of the death certificate for deaths that occurred during the calendar year 2020.
This excerpt explains how death certificates are filled out and how causes are to be listed. Here is an example death certificate to clear up any confusion.

Does everyone remember the NVSS COVID-19 Alert No. 2 mentioned in the first section? For additional reference, this alert was issued on March 24th, 2020. Here’s an excerpt from this alert issued by the NVSS:
The underlying cause depends upon what and where conditions are reported on the death certificate. However, the rules for coding and selection of the underlying cause of death are expected to result in COVID-19 being the underlying cause more often than not.
COVID-19 should be reported on the death certificate for all decedents where the disease caused or is assumed to have caused or contributed to death. Certifiers should include as much detail as possible based on their knowledge of the case, medical records, laboratory testing, etc. If the decedent had other chronic conditions such as COPD or asthma that may have also contributed, these conditions can be reported in Part II.


According to the COVID-19 Alert No. 2: the rules for coding and selection involving the underlying cause of death, COVID-19 is expected to be the underlying cause of death more often than not? They literally advised healthcare providers to ASSUME that if Covid is present, Covid is the underlying cause of death WITHOUT any methods of verification. Does this sound like an accurate method of reporting?
On April 14th, the CDC changed the medical criteria for diagnosis solely for Covid-19 based on the CSTE Covid-19 position paper. The NVSS issued this notice to healthcare providers regarding guidance for certifying deaths due to Covid-19:
If COVID–19 played a role in the death, this condition should be specified on the death certificate. In many cases, it is likely that it will be the UCOD, as it can lead to various life-threatening conditions, such as pneumonia and acute respiratory distress syndrome (ARDS). In these cases, COVID–19 should be reported on the lowest line used in Part I with the other conditions to which it gave rise listed on the lines above it.
When a death is due to COVID–19, it is likely the UCOD and thus, it should be reported on the lowest line used in Part I of the death certificate. Ideally, testing for COVID–19 should be conducted, but it is acceptable to report COVID–19 on a death certificate without this confirmation if the circumstances are compelling within a reasonable degree of certainty.

This guidance shows how Covid should be listed in Part I of a death certificate in most cases. But then proceeds to state, that it is acceptable to report Covid as the underlying cause of death WITHOUT testing confirmation? To what degree does listing Covid as the underlying cause of death WITHOUT testing confirmation remotely make sense? This implies an individual could die from natural causes but since they had a runny nose, it should be assumed they died from Covid. To what degree has the data been manipulated by hospitals?
Let’s recap: The ICD-10 code for Covid is U07.1. In 2020, 5.5% of death certificates only had the code U07.1 listed as the underlying cause of death and 94.5% of death certificates had more than one code assigned to them. On a death certificate the underlying cause of death is listed on Part I. The NVSS COVID-19 Alert No. 2 states that Covid will be assumed to be the underlying cause more often than not, without methods of verification. The guidance issued by the NVSS for the certification of Covid deaths states that without testing confirmation, it is acceptable to list Covid as an underlying cause of death? Starting to see the possibility that the numbers are intentionally being inflated?
Death Certificate Issues:
An article published on September 18th, 2021 in Just the News, highlighted two Colorado officials warning of the inflation of Covid death statistics. The article includes excerpts from interviews with Grand County coroner Brenda Bock and James Caruso, the chief medical examiner and coroner for Denver. The statements made by both coroners’ provide validity behind the possibility of Covid death statistics being highly inflated.
I was told by some of my fellow coroners in the more rural counties in Colorado that it was happening to them, that they knew of issues where they had signed out a death certificate with perhaps trauma involved. And they were being advised that it was being counted as a COVID-related death.
I think early on, the people signing the death certificates probably were doing it accurately. But at some level — maybe the state level, maybe the federal level — there's a possibility that they were cross-referencing COVID tests. And that people who tested positive for COVID were listed as a COVID-related death, regardless of their true cause of death. And I believe that's very erroneous, and not the way the statistics needed to be accumulated.
I believe they're very inflated. And don't get me wrong. I believe COVID is real. And I believe people do get very sick from it. And I do believe a small number do die from that.
As coroner, when we are elected, our job is to find out the reason someone died. It's the truth. I'm not going to falsify a death certificate because my job is to tell the truth about why a person died, the cause and the manner. And I don't believe that what's going on is the truth.
The comments made by the coroners are quite shocking and are first hand accounts of the inflation and manipulation of Covid death statistics. This is happening all around the country, unfortunately the extent of which is unknown.
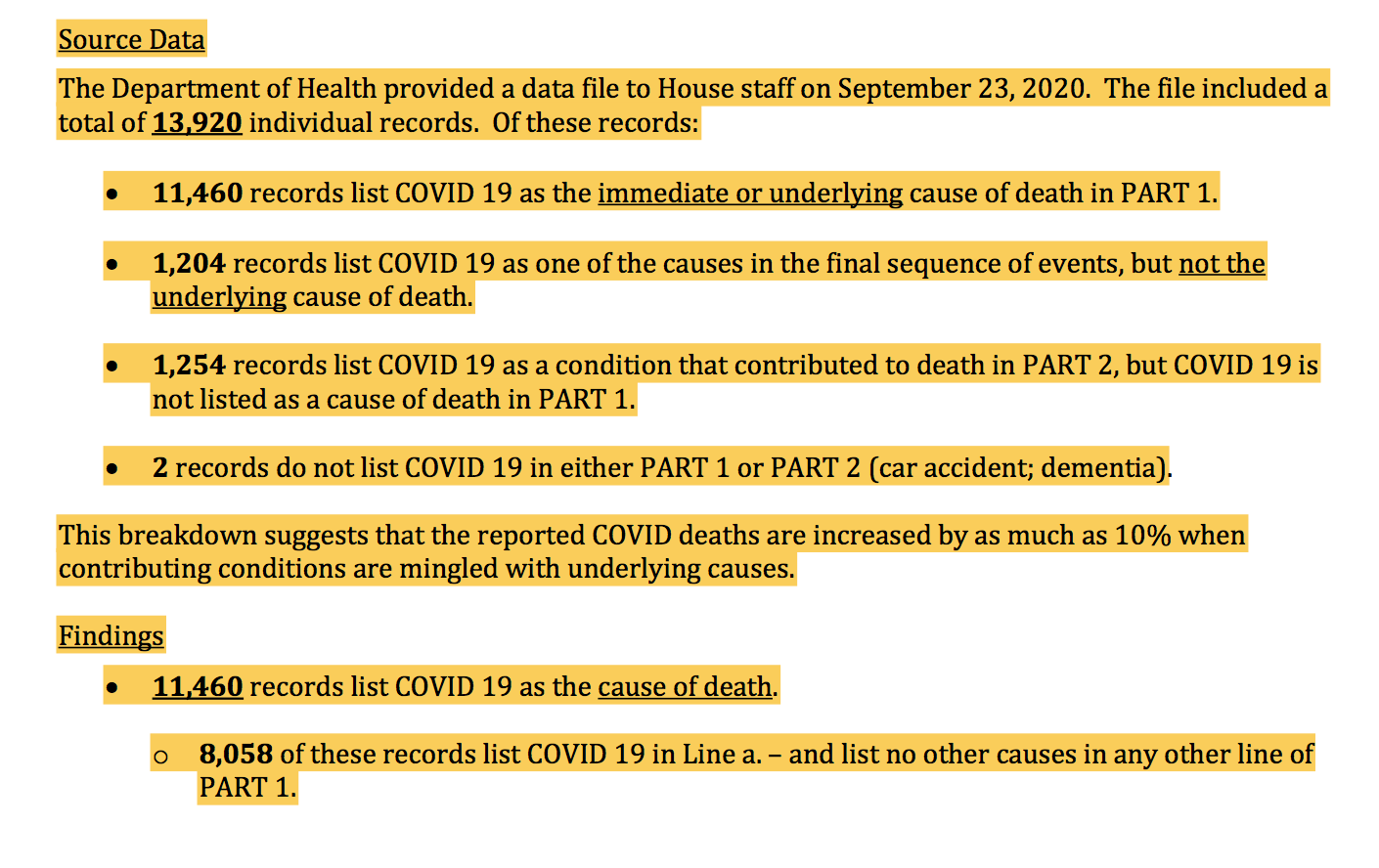
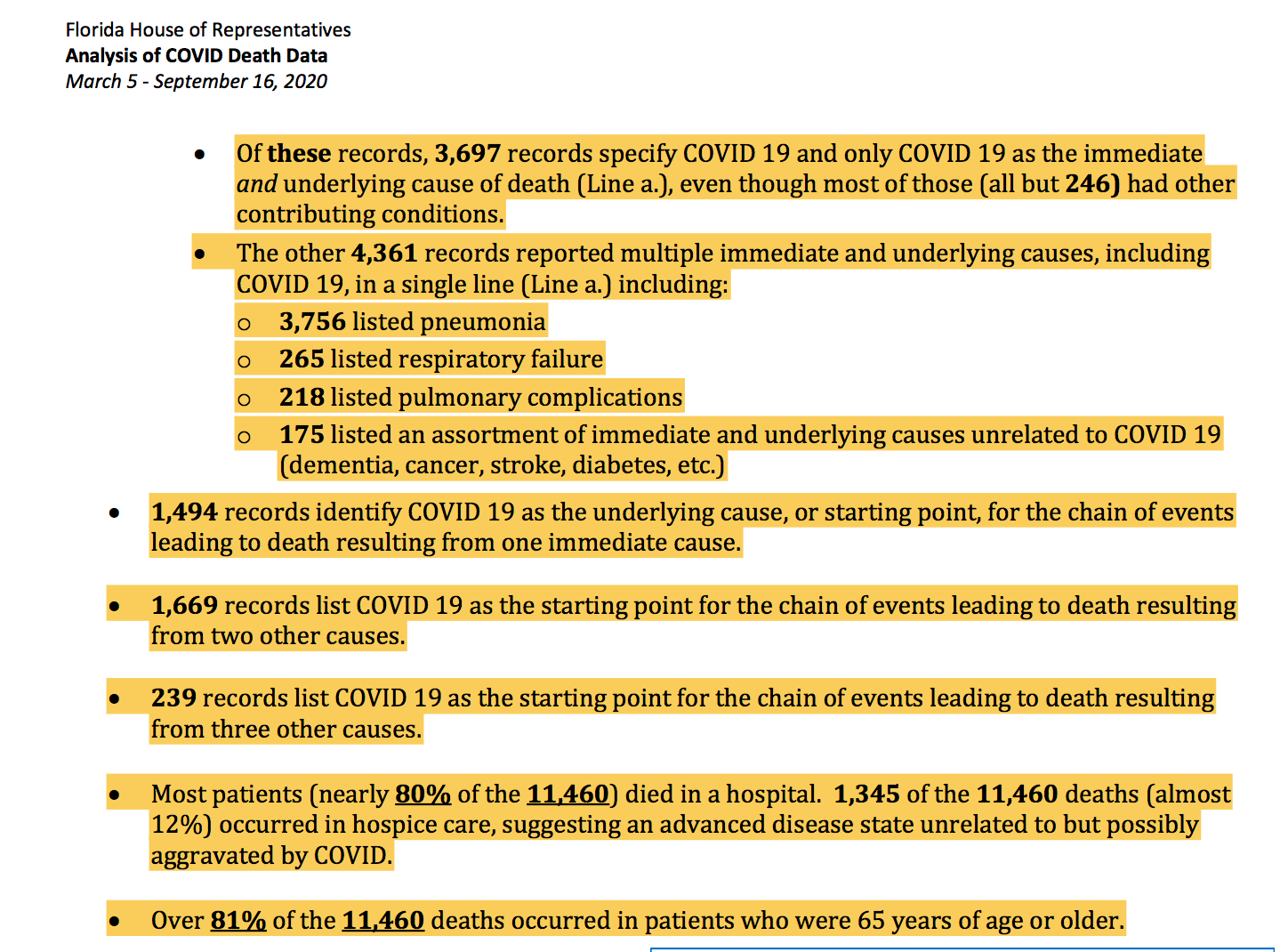
An article from November 2020, highlighted the results from an examination of death certificates in Florida. The findings from this examination led to a multitude of questions that surround the validity of the official number of Covid deaths. Florida House Speaker Jose Oliva’s staff produced an Analysis of COVID Death Data report on October 12th, which reviewed 13,920 death certificates provided by the Florida Department of Health.
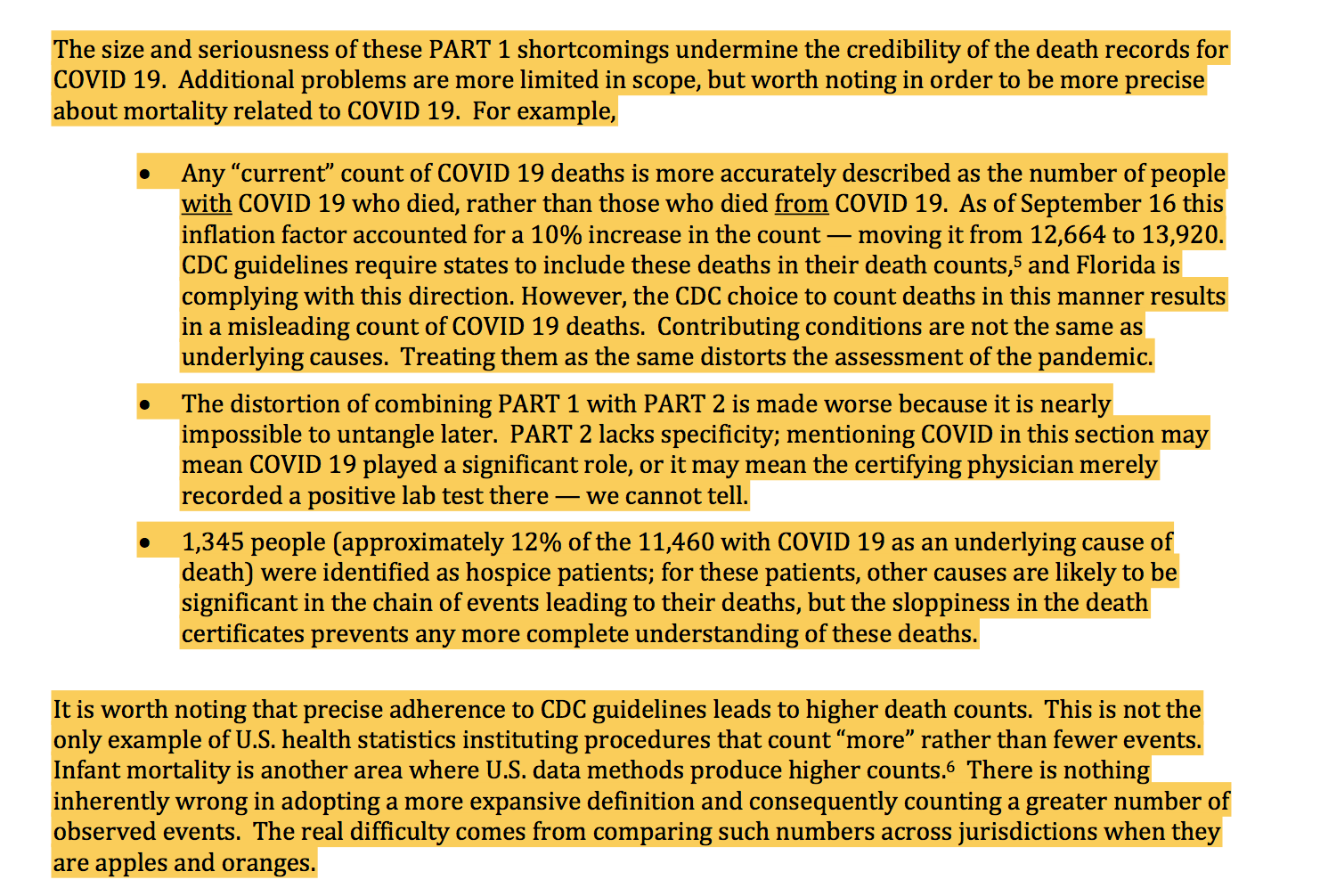
This breakdown suggests that the reported COVID deaths are increased by as much as 10% when contributing conditions are mingled with underlying causes.
Nearly 60% of the records classified by the Department of Health have errors or are recorded in a manner inconsistent with state and national guidance. The problematic records (8,058 of them) only provide underlying cause of death information in Line a. of PART 1. Of these, 7,629 were completed by medical examiners.
Any “current” count of COVID 19 deaths is more accurately described as the number of people with COVID 19 who died, rather than those who died from COVID 19. As of September 16 this inflation factor accounted for a 10% increase in the count — moving it from 12,664 to 13,920. CDC guidelines require states to include these deaths in their death counts,5 and Florida is complying with this direction. However, the CDC choice to count deaths in this manner results in a misleading count of COVID 19 deaths. Contributing conditions are not the same as underlying causes. Treating them as the same distorts the assessment of the pandemic.

Unfortunately, the true number of Covid positive cases that have occurred will never be determined. On the contrary, the true number of deaths can be calculated from the ICD-10 death codes associated with death certificates. One would count the number of death certificates that only have the Covid ICD-10 code assigned (U07.1), then count the number of death certificates that have U07.1 and at least one other ICD-10 code assigned, then compare to the total number listed for the given area. Next, the examination of all death certificates would also have to be conducted in order to cross reference the ICD-10 codes, in order to conclusively determine the true number of deaths. The method in which death certificates are filled out is also imperative for accuracy, as seen in the Florida House Analysis of COVID-19 deaths. Given the CDC’s unprecedented decision to alter the reporting guidelines exclusively for Covid, one can assume that the death totals are inflated. How can any official honestly claim the numbers presented are accurate due to the unprecedented changes in reporting guidelines exclusively for Covid related deaths and discrepancies shown on death certificates?
Prevalence of Co-Morbidities in Covid Deaths:
This section will include two studies that were included in part 3 of my Truth About Covid mini-series. I am including these two studies to further show the prevalence of underlying conditions playing a major contributing role in Covid related deaths and hospitalizations. Make note of the specifics surrounding death certificates and how other factors are actively playing a role in the death count. These studies further illustrate the obscurity associated with Covid related death totals.
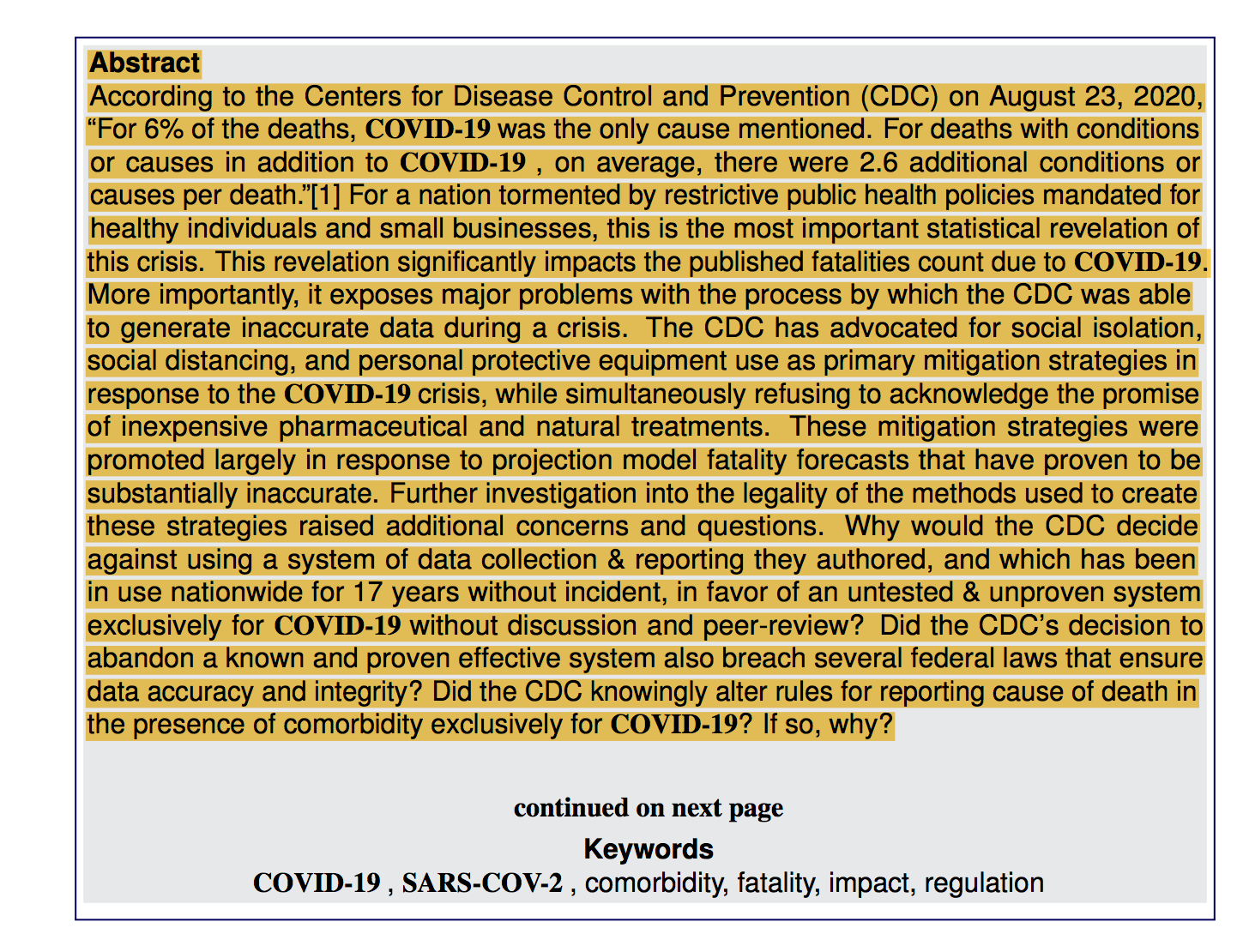
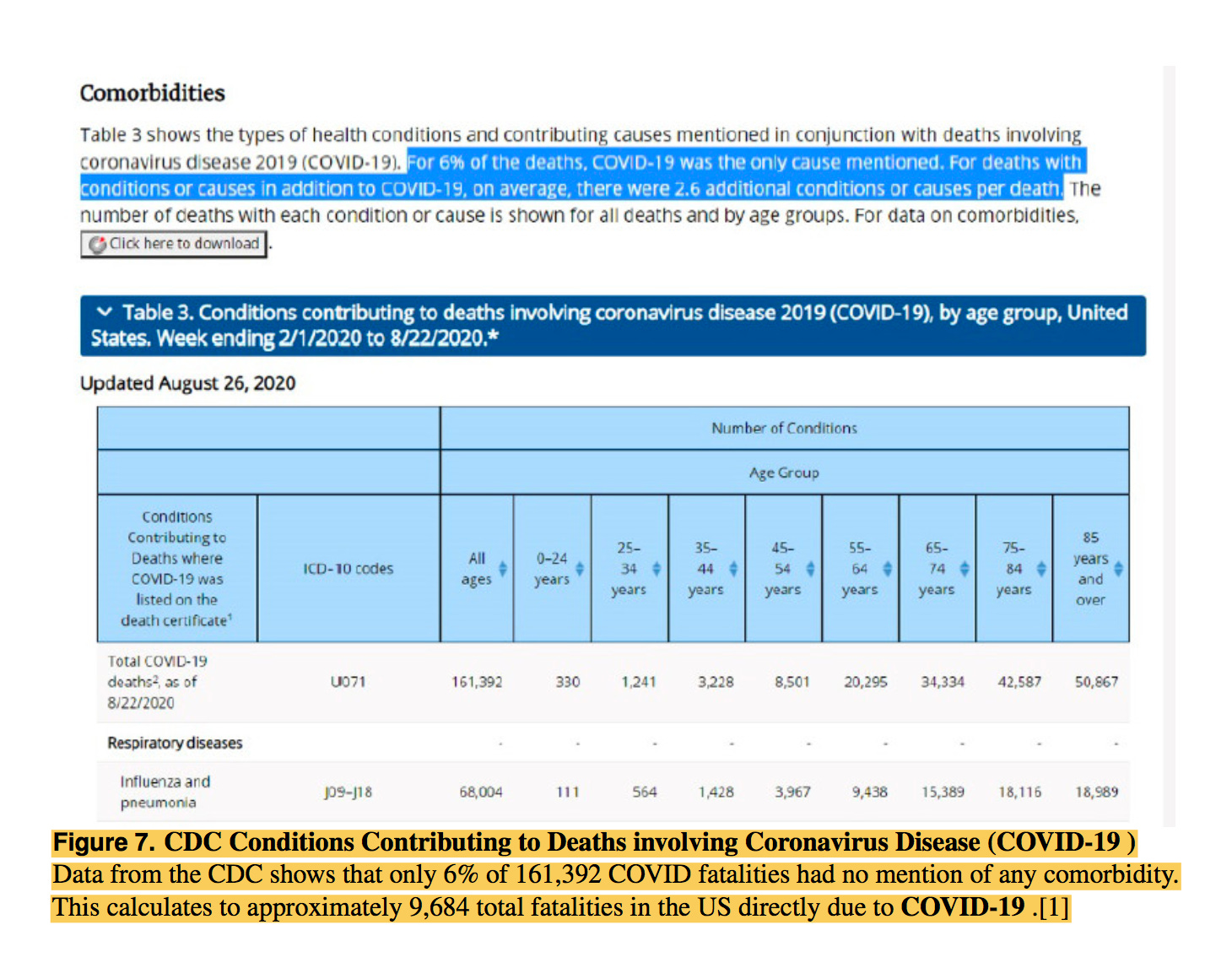
The Institute for Pure & Applied Knowledge published a study that analyzed the prevalence of co-morbidities in Covid related deaths. The study also highlighted the inadequacies of the CDC’s reporting guidelines for Covid as compared to the 2003 reporting guidelines used by the CDC. In August of 2020, the CDC quietly admitted only 6% of Covid related deaths listed at this time, had “Covid” listed as the sole cause of death. Until August, 94% of listed Covid deaths had an average of 2.6 underlying conditions that contributed to the cause of death.
Institute for Pure & Applied Knowledge: Covid Data Collection, Comorbidity & Federal Law: A Historical Perspective
According to the Centers for Disease Control and Prevention (CDC) on August 23, 2020, “For 6% of the deaths, COVID-19 was the only cause mentioned. For deaths with conditions or causes in addition to COVID-19 , on average, there were 2.6 additional conditions or causes per death.
The CDC published guidelines on March 24, 2020 that substantially altered how cause of death is recorded exclusively for COVID-19. This change was enacted apparently without public opportunity for comment or peer-review. As a result, a capricious alteration to data collection has compromised the accuracy, quality, objectivity, utility, and integrity of their published data, leading to a significant increase in COVID-19 fatalities.
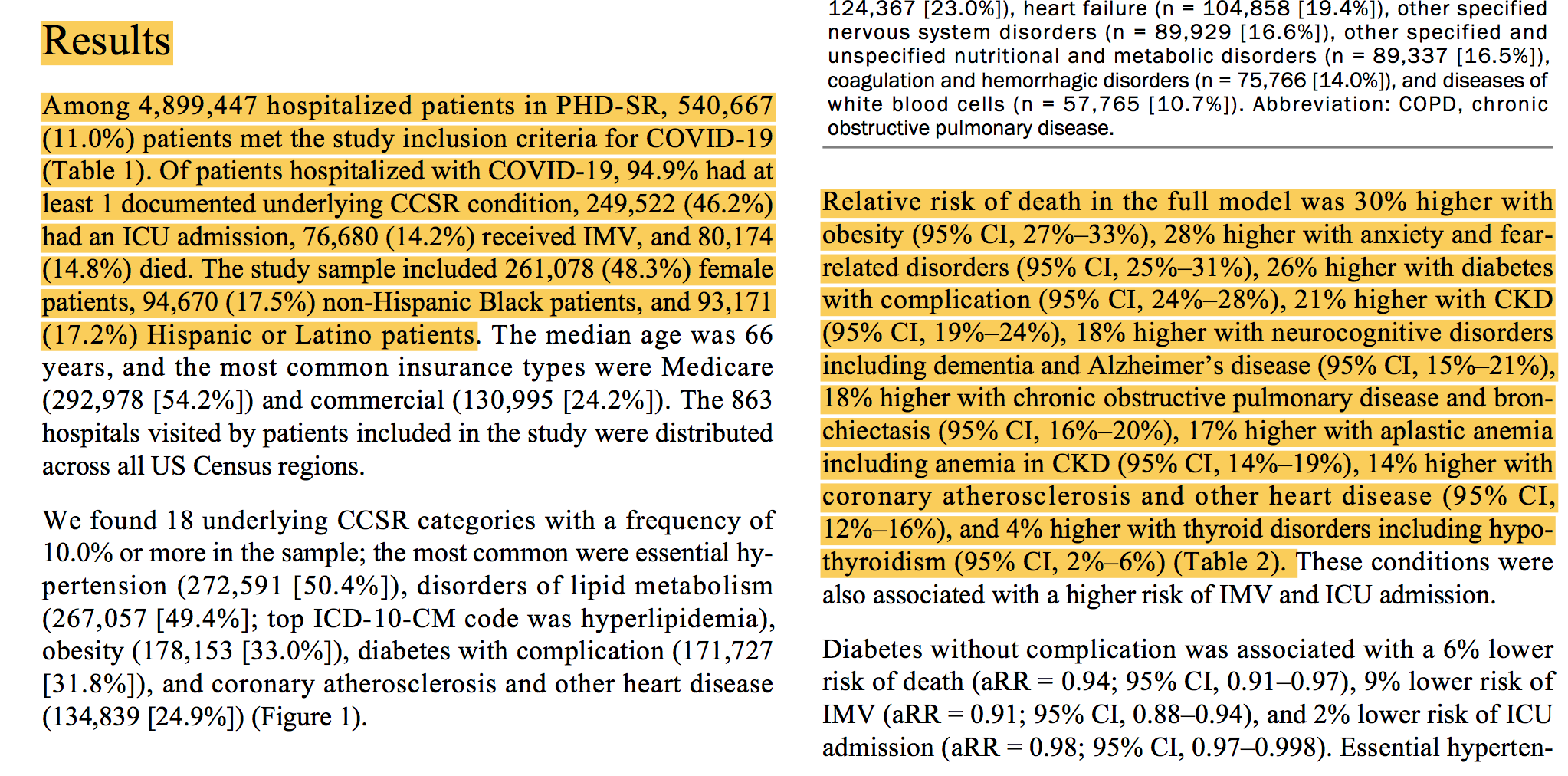
A study from the CDC analyzed how co-morbidities and disease have played a role in the increased prevalence of hospitalizations associated with a Covid infection. From March 2020-March 2021, 540,667 adults were hospitalized with Covid complications. Out of the number of adults hospitalized during this time frame, 94.9% of which had at least one medical condition. The most common underlying conditions were essential hypertension, disorders of lipid metabolism, and obesity. Of the most common conditions found, obesity had the strongest risk factor associated with death.
Preventing Chronic Disease-Public Health, Research, Practice & Policy: Underlying Medical Conditions & Severe Illness Among 540,667 Adults Hospitalized With Covid-19, March 2020-March 2021
Among 4,899,447 hospitalized adults in PHD-SR, 540,667 (11.0%) were patients with COVID-19, of whom 94.9% had at least 1 underlying medical condition. Essential hypertension (50.4%), disorders of lipid metabolism (49.4%), and obesity (33.0%) were the most common.
Certain underlying conditions and the number of conditions were associated with severe COVID-19 illness. Hypertension and disorders of lipid metabolism were the most frequent, whereas obesity, diabetes with complication, and anxiety disorders were the strongest risk factors for severe COVID-19 illness.

These studies show that Covid deaths and hospitalizations have a direct correlation with prior medical conditions. Individuals that have underlying issues are more susceptible to severe illness and even death with various diseases, not just Covid. The lack of healthy dietary habits and lack of exercise in the country as a whole, is the driving factor behind over a million deaths on a yearly basis. If we addressed these issues, the quality of health would substantially increase throughout the country. I included these studies because they show a multitude of health issues associated with Covid related death and severe illness. These studies also help highlight the increased possibility of Covid deaths actually being caused from various issues other than Covid itself. The prevalence of prior medical conditions listed on death certificates, imply a number of individuals could have actually died from other causes but happened to test “positive” for Covid while at the hospital. This is why I emphasized the difference between ‘with’ and ‘from.’ If an individual died WITH Covid, this does not mean the underlying cause of death was Covid, which is significantly different than if an individual dies FROM Covid. By design, these distinctions have been intentionally blurred by officials.
CDC’s “Hidden” PIC Data:
The Covid Tracking Project by the CDC and Johns Hopkins, has done an excellent job at “hiding” Covid related data, which has made trying to understanding the data extremely difficult. The CDC’s weekly report update by week and state, lacks a sole column for deaths from Covid only. They have combined data into various columns such as: Deaths involving Pneumonia, with or without COVID-19, excluding Influenza deaths and All Deaths involving Influenza, with or without COVID-19 or Pneumonia. Just to provide a few examples. This creates major discrepancies within the data and how it should be interpreted. Given the broad column headings for the PIC data, how does one attempt to interpret this data? How does one determine if the deaths were caused from influenza, pneumonia or Covid? Conveniently, the CDC suspended data collection for the 2020-2021 influenza season in May of 2020 which showed the geographic spread of influenza.
Below is the Deaths involving COVID-19, pneumonia and influenza or PIC data.
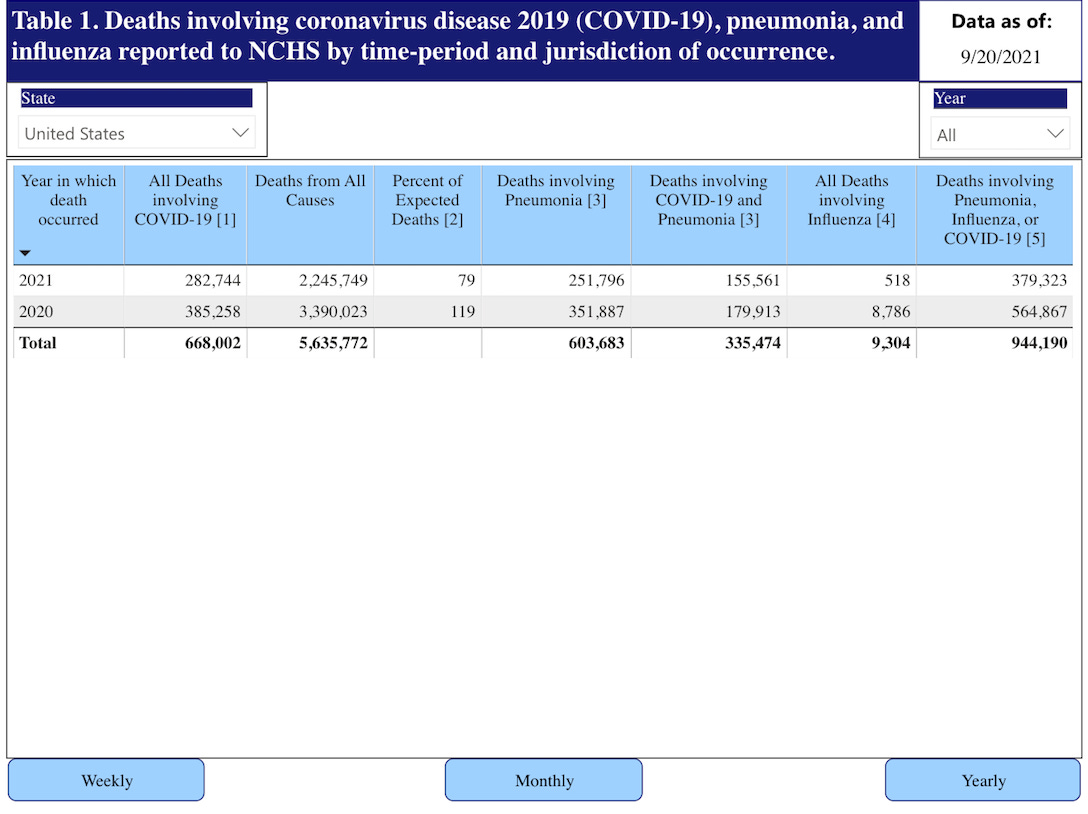

As you can see, attempting to understand the data is rather difficult due to the lack of a “Deaths from COVID-19” only column. The CDC has lumped together ALL deaths involving COVID-19, which makes the data unreliable because of the implication that any cause of death listed in these columns is considered a “COVID-19” death. Combining influenza, pneumonia and Covid deaths implies we cannot determine the true cause of death, thus skews the data. The manipulation of data is a serious issue which has led to the inflation of death totals and hospitalization numbers.
The Disappearance of the Flu:
The Covid pandemic has resulted in a multitude of scientific anomalies but, one of the most peculiar is the disappearance of the seasonal flu. Influenza is a respiratory virus that humans have dealt with for over 100 years. The typical flu season begins in October and can last up until late May, usually 6-8 months in total duration.
Influenza is defined as:
Usually referred to as the flu or grippe, influenza is a highly infectious respiratory disease. The disease is caused by certain strains of the influenza virus. When the virus is inhaled, it attacks cells in the upper respiratory tract, causing typical flu symptoms such as fatigue, fever and chills, a hacking cough, and body aches. Influenza victims are also susceptible to potentially life-threatening secondary infections.
To provide some historical context, here is an overview of flu seasons from 2010-2020:
2010-11: 21,000,000 cases, 290,000 hospitalizations, 37,000 deaths
2011-12: 9,300,000 cases, 140,000 hospitalizations, 12,000 deaths
2012-13: 34,000,000 cases, 570,000 hospitalizations, 43,000 deaths
2013-14: 30,000,000 cases, 350,000 hospitalizations, 38,000 deaths
2014-15: 30,000,000 cases, 590,000 hospitalizations, 51,000 deaths
2015-16: 24,000,000 cases, 280,000 hospitalizations, 23,000 deaths
2016-17: 29,000,000 cases, 500,000 hospitalizations, 38,000 deaths
2017-18: 45,000,000 cases, 810,000 hospitalizations, 61,000 deaths
2018-19: 36,000,000 cases, 490,000 hospitalizations, 34,000 deaths
2019-20: 38,000,000 cases, 400,000 hospitalizations, 22,000 deaths
2020-21: 1,675 cases, no data on hospitalizations, no data on deaths
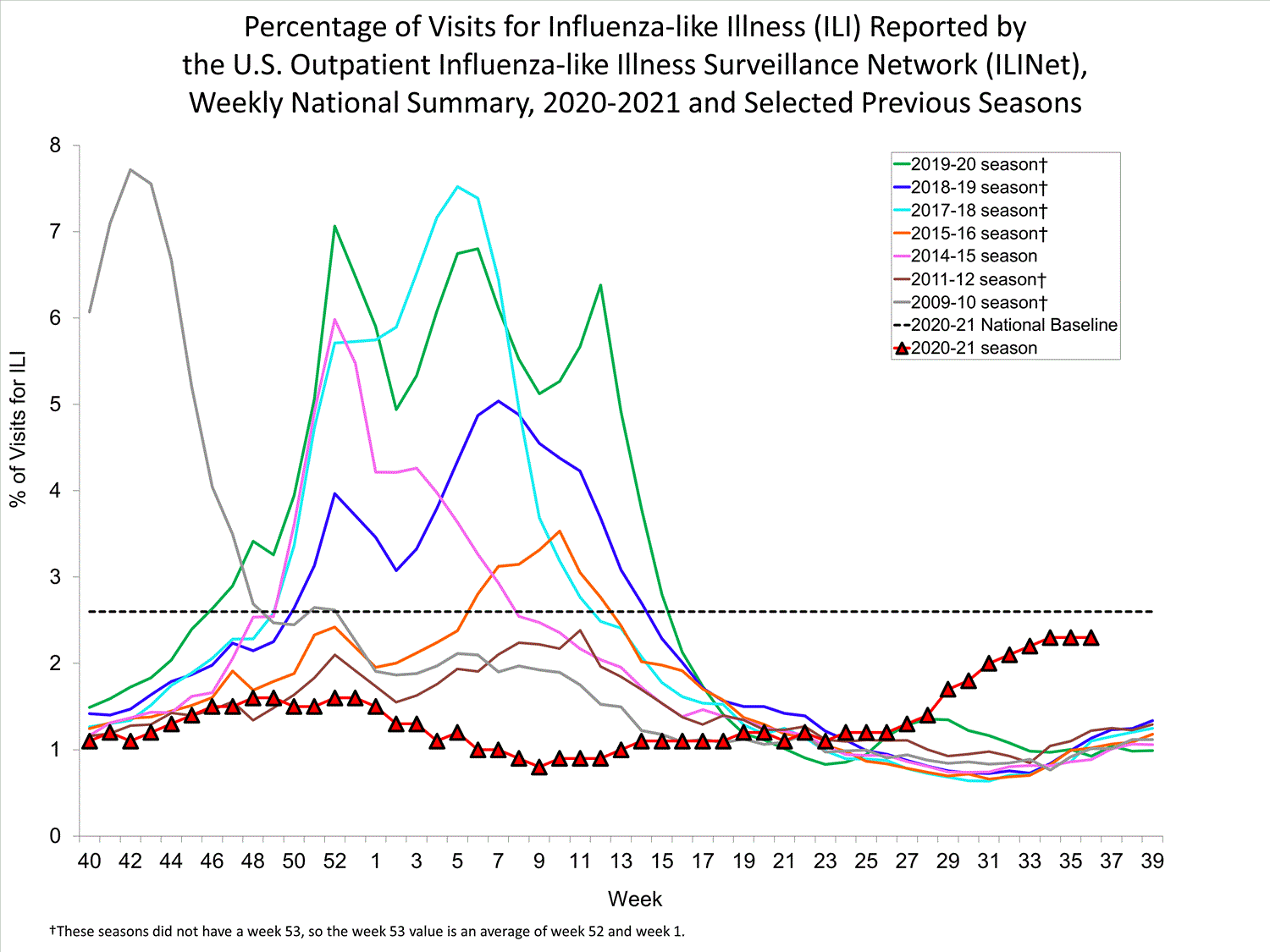

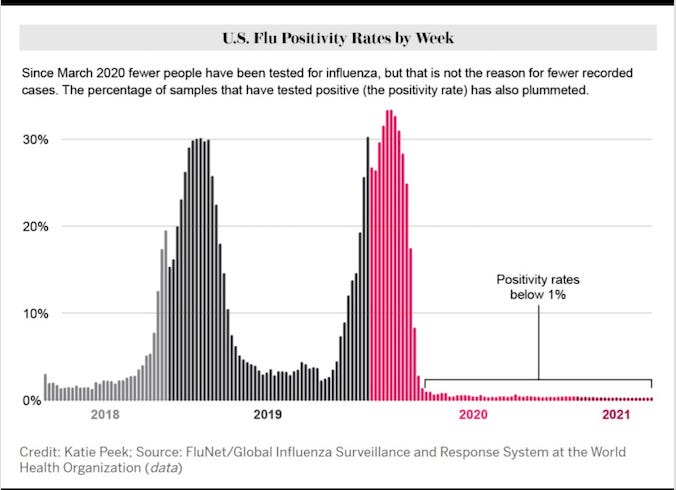
As you can see, the 2017-2018 flu season was significantly worse than any flu season in the last 10+ years. The number of cases, hospitalizations and deaths were the highest during this timeframe. We can also see that the flu was virtually non-existent during the 2020-2021 season. What would be the driving factor behind the flu positivity rate going from exponentially high to virtually obsolete? In one year we had a decrease of almost 38 million flu cases, does that make any sense? Don’t forget, the CDC conveniently suspended data collection for the flu in May of 2020.
To further provide perspective, the United States has a total of 6,090 hospitals across the country and the total number of staffed beds is 919,559. Hospitalizations in the country didn’t exceed 60,000 in one day until November 10th, 2020.
March 31st, 2020 total cumulative Covid positive hospitalizations: 23,725
April 30th, 2020 total cumulative Covid positive hospitalizations: 123,786
July 31st, 2020 total cumulative Covid positive hospitalizations: 308,088
September 30th, 2020 total cumulative Covid positive hospitalizations: 408,649
November 17th, 2020 total cumulative Covid positive hospitalizations: 517,471
The total number of Covid positive hospitalizations from January 20th-November 17th was 517,471. In those 10 months, we actually had less hospitalizations due to Covid than the 2012-2013, 2014-2015, and 2017-2018 flu seasons respectively. In the year 2018 alone, 36,251,159 people were admitted to hospitals around the country. In the 2017-2018 flu season, (6-8 month timeframe) we had roughly 810,000 hospitalizations due to the flu. Does anyone recall hearing about that on the news or the imposition of lockdowns being considered? What the CDC and the media didn’t tell you, was that over 70% of Covid hospitalizations recovered and 49.49% of all Covid related deaths included pneumonia. They also fail to mention that over 40% of Covid related deaths occurred in long term health facilities and nursing homes (Cuomo, Whitmer, Newsom, Murphy & Wolf). The entire premise behind lockdowns was to ensure hospitals didn’t get overrun. What they failed to mention was that our hospital system is very capable of handling mass amounts of patients as seen in previous years. The emphasis of “hospitals are overrun” was to instill fear and maintain control over the population and we are seeing that being emphasized again today. Between October and November they will use the same guise that hospitals are overrun, in order to usher in a new round of lockdowns. Just watch. Hint: it will be due to ADE caused by the vaccine, the data from Israel proves this given the timing of vaccine rollouts.
A rational individual would see the data presented in this section and begin to scratch one’s head in confusion. The disappearance of the flu is an anomaly that cannot be explained by anything other than flu cases having been considered Covid cases, due to the PCR tests inability to decipher between the two illnesses. I presented this information to further provide perspective behind Covid numbers being intentionally inflated in order to maintain control and fear over the population. Given the CDC’s suspension of flu related data on May 20th, we have no way to determine the true number of Covid cases and true number of those that had the flu instead. The lack of transparency and constant hysteria has created a dangerous precedent going forward within the medical community. The blatant disregard for accuracy and transparency has resulted in a loss of faith in our medical system and healthcare employees.
Final Points:
This article highlighted the unprecedented changes made by the CDC, in regards to how deaths are to be reported exclusively for Covid and how these changes have led to a significant possibility of Covid death totals being inflated. Understanding the process in which deaths are reported, is important in the attempt to make sense of the numbers presented to the public. Given the information about the reporting guidelines, ICD-10 codes, PIC data, and underlying medical conditions associated with Covid deaths, one can draw the conclusion that the death totals have been heavily inflated. The blatant inaccuracy of Covid statistics is (by design) to instill fear within the general population. A multitude of discrepancies lie within the data the CDC has provided to the public and need to be addressed. Although we will never know a true case count for Covid, figuring the true death count is a significant possibility. My assumption is that Covid is responsible for roughly 100,000 deaths at most but that is pure speculation. This article is very technical and data driven but the information provided is valuable when trying to understand how to articulate the numbers provided by the CDC. I hope this article provided insight behind the inaccuracies in the reporting of numbers associated with Covid and how the facts point to the numbers being heavily inflated. Understanding how to articulate the data associated with Covid is imperative when trying to make sense of everything going on. If you can see the issues associated with the numbers everything else will begin to make more sense. I doubt we will ever truly know the extent of the inaccuracies associated with Covid numbers but understanding that it’s the reality of the situation is vitally important to understanding what’s truly happening.